Arterial gipertenziya
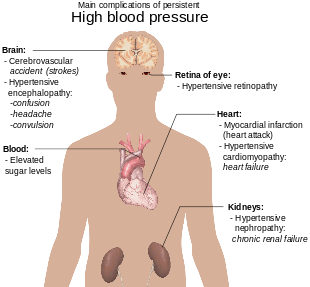
Gipertenziya (HTN yoki HT), shuningdek, yuqori qon bosimi (HBP) sifatida ham tanilgan, arteriyalarda qon bosimi doimiy ravishda koʻtarilgan uzoq muddatli tibbiy holatdir[1]. Uzoq muddatli yuqori qon bosimi insult, koronar arteriya kasalligi, yurak yetishmovchiligi, atriyal fibrilatsiya, periferik arterial kasalliklar, koʻrish qobiliyatini yoʻqotish, surunkali buyrak kasalligi va demans uchun asosiy xavf omilidir[2][3][4][5]. Gipertenziya butun dunyo boʻylab erta oʻlimning asosiy sababidir[6].
Yuqori qon bosimi birlamchi (asosiy) yoki ikkilamchi gipertenziya deb tasniflanadi[7]. Taxminan 90-95 % holatlar birlamchi boʻlib, oʻziga xos boʻlmagan turmush tarzi va genetik omillar tufayli yuqori qon bosimi sifatida aniqlanadi[7][8]. Kasallik xavfni oshiradigan turmush tarzi omillari orasida dietada ortiqcha tuz, ortiqcha tana vazni, chekish va spirtli ichimliklarni tartibsiz isteʼmol qilish natijasida yuzaga keladi[9][7]. Qolgan 5-10 % hollarda surunkali buyrak kasalligi, buyrak arteriyalarining torayishi, endokrin kasalliklar yoki tugʻilishni nazorat qilish tabletkalarini qoʻllash kabi aniqlanganligi tufayli, yuqori qon bosimi sifatida tavsiflangan ikkilamchi yuqori qon bosimi deb tasniflanadi[7].
Qon bosimi ikkita oʻlchov boʻyicha tasniflanadi: sistolik va diastolik bosim. Mos ravishda maksimal va minimal bosimdir[9]. Koʻpgina kattalar uchun dam olishda normal qon bosimi sistolik simob (mmHg) 100-130 millimetr va diastolik 60-80 mmHg oraligʻida yuz beradi[10][11]. Aksariyat kattalar uchun qon bosimi doimiy ravishda 130/80 yoki 140/90 mmHg dan yuqori boʻlsa, yuqori qon bosimi mavjud deb hisoblanadi[7][10]. Bolalar uchun turli raqamlar qoʻllanadi[12].
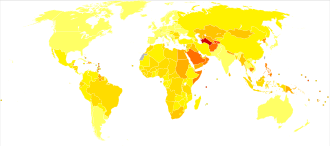
Turmush tarzini oʻzgartirish va dori-darmonlar qon bosimini pasaytirishi va sogʻliq uchun asoratlar xavfini kamaytirishi mumkin[13]. Turmush tarzi oʻzgarishi vazn yoʻqotish, jismoniy mashqlar, tuz isteʼmolini kamaytirish, spirtli ichimliklarni isteʼmol qilishni kamaytirish va sogʻlom ovqatlanishni oʻz ichiga oladi[7]. Agar turmush tarzini oʻzgartirish yetarli boʻlmasa, u holda qon bosimida dori vositalari qoʻllanadi[13]. Bir vaqtning oʻzida qabul qilingan uchta dori 90 % odamlarda qon bosimini nazorat qila oladi[7]. Oʻrtacha yuqori arterial qon bosimini (>160/100 mmHg sifatida aniqlanadi) dori vositalari bilan davolash umr koʻrish davomiyligini oshirish bilan bogʻliq[14]. Qon bosimini davolashning taʼsiri 130/80 orasida mmHg va 160/100 mmHg unchalik aniq emas. Yuqori qon bosimi butun dunyo aholisining 16 dan 37 foizigacha taʼsir qiladi[7]. 2010-yilda 18 foiz oʻlimga gipertenziya sabab boʻlgani aniqlandi. Dunyo boʻyicha 9,4 million kishi aynan gipertenziyadan vafot etadi[15].
Belgilari va belgilari
tahrirGipertenziya kamdan-kam hollarda alomatlar bilan birga keladi va uni aniqlash odatda skrining orqali yoki bogʻliq boʻlmagan muammo uchun tibbiy yordam soʻrab murojaat qilganda amalga oshiriladi. Qon bosimi yuqori boʻlgan baʼzi odamlar bosh ogʻrigʻi (ayniqsa, ertalab boshning orqa qismidagi ogʻrigʻi) shuningdek, bosh aylanishi, bosh aylanishi, tinnitus (quloqlarda shovqin yoki shivirlash), koʻrishning oʻzgarishi yoki hushidan ketish mumkin[16]. Jismoniy tekshiruvda gipertenziya oftalmoskopiya bilan koʻrilgan optik fundusdagi oʻzgarishlar mavjudligi bilan bogʻliq boʻlishi mumkin[17]. Gipertenziv retinopatiyaga xos boʻlgan oʻzgarishlarning zoʻravonligi I dan IV darajagacha; I va II darajalarni farqlash qiyin boʻlishi mumkin[17].
Ikkilamchi gipertenziya
tahrirIkkilamchi gipertenziya aniqlangan sababga koʻra gipertenziya boʻlib, maʼlum oʻziga xos qoʻshimcha belgilar va alomatlarga olib kelishi mumkin[18]. Gipertiroidizm tez-tez ishtahaning kuchayishi, tez yurak urishi, koʻzlarning shishishi va titroq bilan vazn yoʻqotishiga olib keladi. Buyrak arteriyasi stenozi (RAS) oʻrta chiziqning chap yoki oʻng tomonida (bir tomonlama RAS) yoki ikkala joyda (ikki tomonlama RAS) mahalliylashtirilgan qorin boʻshligʻi bilan bogʻliq boʻlishi mumkin. Aorta koarktatsiyasi koʻpincha qoʻllarga nisbatan pastki ekstremitalarda qon bosimining pasayishiga yoki femoral arterial pulslarning kechikishi yoki yoʻqligiga olib keladi. Feokromotsitoma bosh ogʻrigʻi, yurak urishi, rangpar koʻrinish va ortiqcha terlash bilan birga keladigan keskin gipertenziya epizodlarini keltirib chiqarishi mumkin[18].
Gipertenziv inqiroz
tahrirYuqori koʻtarilgan qon bosimi (sistolik 180 yoki diastolik 110 ga teng yoki undan yuqori) gipertenziv inqiroz deb ataladi[19]. Gipertenziv inqiroz mos ravishda oxirgi organlarning shikastlanishi yoʻqligi yoki mavjudligiga qarab gipertonik shoshilinch yoki gipertonik favqulodda deb tasniflanadi[20][21]. Shoshilinch gipertenziyada qon bosimining koʻtarilishi natijasida oxirgi organlarning shikastlanishi haqida hech qanday dalil yoʻq. Bunday hollarda 24 dan 48 soatgacha qon bosimini bosqichma-bosqich pasaytirish uchun ogʻiz orqali yuboriladigan dorilargina yordam bera oladi[22]. Gipertenziv favqulodda vaziyatlarda bir yoki bir nechta organlarga bevosita zarar yetkazilishi haqida dalillar mavjud[23][24]. Eng koʻp taʼsirlangan organlarga miya, buyraklar, yurak va oʻpka kiradi. Ular chalkashlik, uyquchanlik, koʻkrak qafasidagi ogʻriqlar va nafas qisilishi kabi belgilarni keltirib chiqaradi[22]. Gipertenziya bilan bogʻliq favqulodda holatlarda, davom etayotgan organlarning shikastlanishini toʻxtatish uchun qon bosimini tezroq pasaytirish kerak[22].
Homiladorlik
tahrirGipertenziya homiladorlikning taxminan 8-10 foizida uchraydi[18]. 140/90 dan yuqori boʻlgan olti soatlik oraliqda ikkita qon bosimi oʻlchovi mm Hg homiladorlikdagi gipertenziya diagnostikasi hisoblanadi[25]. Homiladorlikdagi yuqori qon bosimi oldingi gipertenziya, homiladorlik gipertenziyasi yoki preeklampsi sifatida tasniflanishi mumkin[26]. Preeklampsi — homiladorlikning ikkinchi yarmida va tugʻruqdan keyingi davrda qon bosimi ortishi va siydikda protein mavjudligi bilan tavsiflangan jiddiy holatlardan biridir[18]. Bu homiladorlikning taxminan 5 foizida uchraydi va butun dunyo boʻylab onalar oʻlimining taxminan 16 foizi uchun javobgardir[18]. Odatda preeklampsida hech qanday alomat yoʻq va u muntazam skrining orqali aniqlanadi. Preeklampsi belgilari paydo boʻlganda, bosh ogʻrigʻi, koʻrishning buzilishi (koʻpincha „chiroqlar“ miltillaydi), qusish, oshqozon ogʻrigʻi va shish paydo boʻladi . Preeklampsiya vaqti-vaqti bilan hayot uchun xavfli boʻlgan eklampsiya deb ataladigan holatga oʻtishi mumkin, bu favqulodda gipertenziya boʻlib, koʻrishning yoʻqolishi, miya shishishi, tutilishlar, buyrak yetishmovchiligi, oʻpka shishi va tarqalgan intravaskulyar koagulyatsiya (qon ivishining buzilishi) kabi bir qator jiddiy asoratlar bilan kechadigan asoratlardir[18][27]. Aytib oʻtish kerakki, homiladorlik gipertenziyasi siydikda protein boʻlmagan homiladorlik davrida yangi boshlangan gipertenziya sifatida tavsiflanadi[26].
Bolalar
tahrirRivojlanmaslik, tutilishlar, asabiylashish, energiya yetishmasligi va nafas olish qiyinlishuvi[28] yangi tugʻilgan chaqaloqlar va yosh bolalarda ham gipertoniya bilan bogʻliq boʻlishi mumkin. Bolalarda gipertenziya bosh ogʻrigʻi, sababsiz asabiylashish, charchoq, rivojlanishning sustlashishi, koʻrishning xiralashishi, burundan qon ketishi va yuz falajiga olib kelishi mumkin[28][29].
Sabablari
tahrirBirlamchi gipertenziya
tahrirGipertenziya genlar va atrof-muhit omillarining murakkab oʻzaro taʼsiridan kelib chiqadi. Qon bosimiga kichik taʼsir koʻrsatadigan koʻplab keng tarqalgan genetik variantlar[30], shuningdek, qon bosimiga katta taʼsir koʻrsatadigan baʼzi noyob genetik variantlar aniqlangan[31]. Shuningdek, genom boʻyicha assotsiatsiya tadqiqotlari (GWAS) qon bosimi bilan bogʻliq 35 ta genetik lokusni (joylashuvni) aniqladi. Qon bosimiga taʼsir qiluvchi ushbu genetik lokuslardan 12 tasi yangi topildi[32]. Ushbu sentinel SNP qon tomir silliq mushaklari va buyrak funksiyasi bilan bogʻliq genlar ichida joylashgan. DNK metilatsiyasi qaysidir maʼnoda umumiy irsiy oʻzgaruvchanlikni bir nechta fenotiplarga bogʻlashga taʼsir qilishi mumkin. Ushbu tadqiqotda 35 sentinel SNP (maʼlum va yangi) uchun oʻtkazilgan yagona variant testi genetik variantlar alohida yoki jami yuqori qon bosimi bilan bogʻliq klinik fenotiplar xavfiga hissa qoʻshishini koʻrsatadi[32]. Gʻarbiy ovqatlanish va turmush tarzi bilan bogʻliq boʻlsa, qon bosimi qarish bilan koʻtariladi va keyingi hayotda gipertoniya boʻlish xavfi katta boʻladi[33][34]. Bir qator atrof-muhit omillari qon bosimiga taʼsir qiladi. Tuzni koʻp isteʼmol qilish tuzga sezgir odamlarda qon bosimini oshiradi; jismoniy mashqlar yetishmasligi, markaziy semizlik alohida holatlarda rol oʻynashi mumkin. Kofein isteʼmoli[35] va D vitamini yetishmovchiligi[36] kabi boshqa omillarning mumkin boʻlgan rollari unchalik aniq emas. Semirib ketishda tez-tez uchraydigan va X sindromining tarkibiy qismi boʻlgan insulin qarshiligi ham gipertenziyaga yordam beradi[37]. Bolaning kam vaznda tugʻilishi, onaning chekishi va emizishning yetishmasligi kabi erta hayotdagi hodisalar kattalar uchun muhim gipertenziya uchun xavf omillari boʻlishi mumkin. Gipertenziya bilan ogʻrigan bemorlarda normal qon bosimi boʻlgan odamlarga nisbatan yuqori qon siydik kislotasi darajasining ortishi aniqlangan, ammo birinchisi sababchi rol oʻynaydimi yoki buyrak funksiyasining yomonlashishiga yordam beradimi, bu savollar noaniqligicha qolmoqda[38]. Qishda oʻrtacha qon bosimi yozga qaraganda yuqori boʻlishi mumkin[39]. Periodontal kasallik ham yuqori qon bosimi bilan bogʻliq[40].
Ikkilamchi gipertenziya
tahrirIkkilamchi gipertenziya aniqlangan sabablardan kelib chiqadi. Buyrak kasalligi gipertenziyaning eng koʻp uchraydigan ikkinchi darajali sababidir[18]. Gipertenziya, shuningdek, Kushing sindromi, gipertiroidizm, hipotiroidizm, akromegaliya, Kon sindromi yoki giperaldosteronizm, buyrak arteriyasi stenozi (ateroskleroz yoki fibromuskulyar displazi), giperokrin[18][41]. Ikkilamchi gipertenziyaning boshqa sabablari orasida esa semizlik, uyqu apneasi, homiladorlik, aorta koarktatsiyasi, qizilmiya oʻtini koʻp isteʼmol qilish, spirtli ichimliklarni koʻp isteʼmol qilish, retsept boʻyicha baʼzi dorilar, oʻsimlik preparatlari va qahva, kokain va metamfetamin kabi stimulyatorlar kiradi[18][42]. Ichimlik suvi orqali mishyak taʼsirining koʻtarilgan qon bosimi bilan bogʻliqligi koʻrsatilgan[43][44]. Depressiya ham gipertoniya bilan bogʻliq edi[45]. Koʻpincha yolgʻizlik ham gepertenziyaga sabab boʻluvchi xavfli omilidir[46]. 2018-yilgi tekshiruv shuni koʻrsatdiki, har qanday alkogol erkaklarda qon bosimini oshiradi, bir yoki ikkitadan ortiq ichimliklar esa ayollarda xavfni oshiradi[47].
Patofiziologiya
tahrir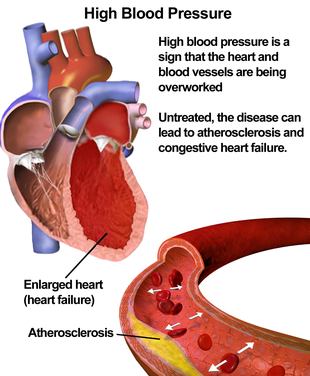
Oʻrnatilgan asosiy gipertenziyasi boʻlgan koʻpchilik odamlarda qon oqimiga qarshilik kuchayishi (umumiy periferik qarshilik) yuqori bosimga olib keladi[48]. Gipertenziyadan oldingi yoki „chegaradagi gipertenziya“ bilan ogʻrigan baʼzi yoshlarda yuqori yurak chiqishi, yurak urish tezligining oshishi va normal periferik qarshilik borligi, giperkinetik chegara gipertenziyasi deb ataladigan dalillar mavjud[49]. Bu odamlar keyingi hayotda oʻrnatilgan asosiy gipertenziyaning tipik xususiyatlarini rivojlantiradilar, chunki ularning yurak faoliyati pasayadi va yosh bilan periferik qarshilik kuchayadi[49]. Oʻrnatilgan gipertenziyada periferik qarshilikning kuchayishi, asosan, mayda arteriyalar va arteriolalarning strukturaviy torayishi bilan bogʻliq[50], ammo kapillyarlar soni yoki zichligining kamayishi ham hissa qoʻshishi mumkin[51]. Gipertenziya, shuningdek, periferik venoz moslashuvning pasayishi bilan bogʻliq[52]. Bu venoz qaytishni oshirishi, yurakning oldingi yukini oshirishi va natijada diastolik disfunksiyani keltirib chiqarishi mumkin. Gipertenziya bilan ogʻrigan keksa odamlarda puls bosimi (sistolik va diastolik qon bosimi oʻrtasidagi farq) tez-tez ortadi[53]. Bu sistolik bosimning anormal darajada yuqori ekanligini anglatishi mumkin, ammo diastolik bosim normal yoki past boʻlishi ham mumkin. Bu holat izolyatsiya qilingan sistolik gipertenziya deb ataladi[54]. Gipertenziya yoki izolyatsiya qilingan sistolik gipertenziya bilan ogʻrigan keksa odamlarda yuqori puls bosimi arterial qattiqlikning oshishi bilan izohlanadi. Bu odatda qarish bilan birga keladi va yuqori qon bosimi bilan kuchayishi mumkin[55]. Gipertenziyada periferik qarshilikning oʻsishini hisobga olish uchun koʻplab mexanizmlar taklif qilingan. Koʻpgina dalillar buyraklardagi tuz va suv bilan ishlashning buzilishini (ayniqsa, intrarenal renin-angiotenzin tizimidagi anormalliklarni)[56] yoki simpatik asab tizimining anormalliklarini nazarda tutadi[57]. Bundan tashqari, endotelial disfunksiya va tomirlarning yalligʻlanishi ham periferik qarshilikning kuchayishiga va gipertenziyadagi tomirlarning shikastlanishiga yordam berishi mumkinligi taxmin qilingan[58][59]. Interleykin 17 oʻsimta nekrozi omili alfa, interleykin 1, interleykin 6 va interleykin 8 kabi gipertenziya bilan bogʻliq deb hisoblangan boshqa immun tizimining kimyoviy signallarini ishlab chiqarishni koʻpaytirishdagi roli uchun qiziqish uygʻotdi[60]. Ratsiondagi ortiqcha natriy yoki kaliyning yetishmasligi ortiqcha hujayra ichidagi natriyga olib keladi. Bu qon tomirlarining silliq mushaklarini qisqartiradi va qon oqimini cheklaydi natijada qon bosimini oshiradi[61][62].
Diagnostika
tahrirAmerika yurak assotsiatsiyasi (AHA) kamida ikkita alohida tibbiy tashrifda kamida uchta dam olish oʻlchovini tavsiya qiladi[63]. Buyuk Britaniyaning Sogʻliqni saqlash va parvarish boʻyicha milliy instituti, agar klinikada qon bosimi 140/90 mmHg yoki undan yuqori boʻlsa, gipertenziya tashxisini tasdiqlash uchun ambulator qon bosimi monitoringini tavsiya qiladi[64].
Oʻlchash texnikasi
tahrirGipertenziyaning aniq tashxisini qoʻyish uchun qon bosimini toʻgʻri oʻlchash texnikasidan foydalanish kerak[65]. Qon bosimini notoʻgʻri oʻlchash tez-tez uchraydi va qon bosimi koʻrsatkichini 10 mmHg ga oʻzgartirishi mumkin, bu esa notoʻgʻri tashxis qoʻyish va gipertenziya notoʻgʻri tasniflanishiga olib keladi[65]. Qon bosimini toʻgʻri oʻlchash texnikasi bir necha bosqichlarni oʻz ichiga oladi. Qon bosimini toʻgʻri oʻlchash uchun qon bosimi oʻlchanayotgan odam kamida besh daqiqa jim oʻtirishni talab qiladi, soʻngra toʻgʻri oʻrnatilgan qon bosimi manjetini yalangʻoch yuqori qoʻliga qoʻyish kerak[65]. Qon bosimi oʻlchanayotgan odam bu jarayonda gaplashmaslik yoki harakat qilmaslik kerak[65]. Oʻlchanayotgan qoʻl yurak darajasida tekis yuzada qoʻllab-quvvatlanishi kerak[65]. Qon bosimini oʻlchash tinch xonada oʻtkazilishi kerak, shuning uchun qon bosimini tekshiradigan shifokor qon bosimini aniq oʻlchash uchun brakiyal arteriyani stetoskop bilan tinglayotganda Korotkoff tovushlarini eshitishi mumkin[65][66]. Korotkoff tovushlarini tinglashda qon bosimi manjetini sekin tushirish kerak (sekundiga 2-3 mmHg)[66]. Biror kishining qon bosimini oʻlchashdan oldin siydik pufagini boʻshatish kerak, chunki bu qon bosimini 15/10 mmHg ga oshirishi mumkin[65]. Toʻgʻriligini taʼminlash uchun bir-biridan 1-2 daqiqa oraliqda bir nechta qon bosimi koʻrsatkichlarini (kamida ikkita) olish kerak[66]. 12-24 soat davomida ambulator qon bosimi monitoringi tashxisni tasdiqlashning eng aniq usuli hisoblanadi[67]. Qon bosimi juda yuqori boʻlganlar bundan mustasno, ayniqsa aʼzolar faoliyati yomonlashganda bu xavfli tus olishi mumkin[68]. 24 soatlik ambulator qon bosimi oʻlchagichlari va uydagi qon bosimi apparatlari mavjudligi tufayli oq xalatli gipertenziya bilan ogʻriganlarga notoʻgʻri tashxis qoʻymaslik muhimligi protokollarning oʻzgarishiga olib keldi. Amerika Qo'shma Shtatlarining profilaktika xizmatlari bo'yicha ishchi guruhi, shuningdek, sogʻliqni saqlash muhitidan tashqarida oʻlchovlarni olishni tavsiya qiladi[67]. Keksa yoshdagi psevdogipertenziya yoki siqilmaydigan arteriya sindromi ham eʼtiborni talab qilishi mumkin. Bu holat arteriyalarning kalsifikatsiyasi bilan bogʻliq boʻlib, natijada qon bosimi manjeti yordamida gʻayritabiiy yuqori qon bosimi koʻrsatkichlari paydo boʻladi, qon bosimining arterial ichidagi oʻlchovlari normaldir[69]. Ortostatik gipertenziya — bu tik turganda qon bosimining oshishi[70].
Boshqa tekshiruvlar
tahrir| Tizim | Testlar | Buyrak | Mikroskopik siydik tahlili, siydikdagi oqsil, BUN, kreatinin | Endokrin | Sarum natriy, kaliy, kaltsiy, TSH | Metabolik | Roʻza qon glyukoza, HDL, LDL, umumiy xolesterin, triglitseridlar | Boshqa | Gematokrit, elektrokardiogramma, koʻkrak qafasi rentgenogrammasi
Gipertenziya tashxisi qoʻyilgach, shifokorlar xavf omillar mavjud boʻlsa, boshqa alomatlar asosida asosiy sababni aniqlashga harakat qilishlari kerak. Ikkilamchi gipertenziya oʻsmirlikdan oldingi bolalarda koʻproq uchraydi. Aksariyat hollarda esa buyrak kasalligi sabab boʻladi. Birlamchi yoki asosiy gipertenziya oʻsmirlar va kattalarda koʻproq uchraydi va koʻplab xavf omillariga, jumladan semirish bilan uzviy bogʻliqdir[77]. Ikkilamchi gipertenziyaning mumkin boʻlgan sabablarini aniqlash va gipertoniya yurak, koʻz va buyraklarga zarar etkazganligini aniqlash uchun laboratoriya tekshiruvlarini ham oʻtkazish mumkin. Qandli diabet va yuqori xolesterin miqdori uchun qoʻshimcha testlar oʻtkaziladi. Hipertansif odamlarni dastlabki baholash toʻliq tarix va fizik tekshiruvni oʻz ichiga olishi kerak. Qon zardobidagi kreatinin miqdori gipertenziya sababi yoki natijasi boʻlishi mumkin boʻlgan buyrak kasalligi mavjudligini aniqlash uchun oʻlchanadi. Buyrak kasalliklarida dietani oʻzgartirish (MDRD) formulasi kabi qoidali tenglamalardan foydalanishni qoʻllab-quvvatlaydi[23]. Bundan tashqari, siydik namunalarini protein uchun tekshirish buyrak kasalligining ikkinchi darajali koʻrsatkichi sifatida ishlatiladi. Elektrokardiogramma (EKG / EKG) yurakning yuqori qon bosimi tufayli zoʻriqishining dalillarini tekshirish uchun amalga oshiriladi. Shuningdek, u yurak mushagining qalinlashuvi (chap qorincha gipertrofiyasi) bor-yoʻqligini yoki yurakda jim yurak xuruji kabi avvalroq kichik buzilishlarni boshdan kechirganligini koʻrsatishi mumkin. Ko'krak qafasi rentgenogrammasi yoki ekokardiyogramma ham yurakning kengayishi yoki yurakning shikastlanishi belgilarini izlash uchun bajarilishi mumkin[18]. Kattalardagi tasnifitahrir
|
|---|

_Venenbild.jpg)
- ↑ Medical sciences, 2, 2014 — 562-bet. ISBN 9780702052491.
- ↑ „Global burden of cardiovascular disease and stroke: hypertension at the core“. The Canadian Journal of Cardiology. 31-jild, № 5. May 2015. 569–571-bet. doi:10.1016/j.cjca.2015.01.009. PMID 25795106.
- ↑ Global atlas on cardiovascular disease prevention and control, 1st, Geneva: World Health Organization in collaboration with the World Heart Federation and the World Stroke Organization, 2011 — 38-bet. ISBN 9789241564373.
- ↑ „Treatment options and considerations for hypertensive patients to prevent dementia“. Expert Opinion on Pharmacotherapy. 18-jild, № 10. July 2017. 989–1000-bet. doi:10.1080/14656566.2017.1333599. PMID 28532183.
- ↑ 5,0 5,1 „Modifiable Risk Factors and Atrial Fibrillation“. Circulation. 136-jild, № 6. August 2017. 583–596-bet. doi:10.1161/CIRCULATIONAHA.116.023163. PMID 28784826.
- ↑ „Hypertension“ (en). www.who.int. Qaraldi: 2022-yil 13-may.
- ↑ 7,0 7,1 7,2 7,3 7,4 7,5 7,6 7,7 „Hypertension“. Lancet. 386-jild, № 9995. August 2015. 801–812-bet. doi:10.1016/s0140-6736(14)61468-9. PMID 25832858.
- ↑ 8,0 8,1 „Essential hypertension. Part I: definition and etiology“. Circulation. 101-jild, № 3. January 2000. 329–335-bet. doi:10.1161/01.CIR.101.3.329. PMID 10645931.
- ↑ 9,0 9,1 „High Blood Pressure Fact Sheet“. CDC (2015-yil 19-fevral). 2016-yil 6-martda asl nusxadan arxivlangan. Qaraldi: 2016-yil 6-mart.
- ↑ 10,00 10,01 10,02 10,03 10,04 10,05 10,06 10,07 10,08 10,09 10,10 10,11 10,12 10,13 10,14 10,15 10,16 10,17 10,18 „2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines“. Hypertension. 71-jild, № 6. June 2018. e13–e115-bet. doi:10.1161/HYP.0000000000000065. PMID 29133356.
- ↑ 11,0 11,1 11,2 11,3 11,4 „2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC)“. European Heart Journal. 34-jild, № 28. July 2013. 2159–2219-bet. doi:10.1093/eurheartj/eht151. PMID 23771844.
- ↑ 12,0 12,1 12,2 12,3 12,4 12,5 „2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8)“. JAMA. 311-jild, № 5. February 2014. 507–520-bet. doi:10.1001/jama.2013.284427. PMID 24352797.
- ↑ 13,0 13,1 „How Is High Blood Pressure Treated?“. National Heart, Lung, and Blood Institute (2015-yil 10-sentyabr). 2016-yil 6-aprelda asl nusxadan arxivlangan. Qaraldi: 2016-yil 6-mart.
- ↑ „Pharmacotherapy for hypertension in adults 60 years or older“. The Cochrane Database of Systematic Reviews. 6-jild. June 2019. CD000028-bet. doi:10.1002/14651858.CD000028.pub3. PMC 6550717. PMID 31167038.
- ↑ „Using the Global Burden of Disease study to assist development of nation-specific fact sheets to promote prevention and control of hypertension and reduction in dietary salt: a resource from the World Hypertension League“. Journal of Clinical Hypertension. 17-jild, № 3. March 2015. 165–167-bet. doi:10.1111/jch.12479. PMC 8031937. PMID 25644474.
- ↑ „Hypertensive vascular disease“, Harrison's Principles of Internal Medicine, 16th, New York: McGraw-Hill, 2005 — 1463–1481-bet. ISBN 978-0-07-139140-5.
- ↑ 17,0 17,1 „The eye in hypertension“. Lancet. 369-jild, № 9559. February 2007. 425–435-bet. doi:10.1016/S0140-6736(07)60198-6. PMID 17276782.
- ↑ 18,00 18,01 18,02 18,03 18,04 18,05 18,06 18,07 18,08 18,09 18,10 18,11 18,12 ABC of hypertension. London: BMJ Books, 2007. ISBN 978-1-4051-3061-5.
- ↑ Research, Center for Drug Evaluation and (2021-01-21). „High Blood Pressure – Understanding the Silent Killer“. FDA (inglizcha).
- ↑ „Hypertensive crisis“. Cardiology in Review. 18-jild, № 2. 2010-04-01. 102–107-bet. doi:10.1097/CRD.0b013e3181c307b7. PMID 20160537.
- ↑ „Hypertensive Crisis“. www.heart.org. 2015-yil 25-iyulda asl nusxadan arxivlangan. Qaraldi: 2015-yil 25-iyul.
- ↑ 22,0 22,1 22,2 „Hypertensive crises: challenges and management“. Chest. 131-jild, № 6. June 2007. 1949–1962-bet. doi:10.1378/chest.06-2490. PMID 17565029. 2012-12-04da asl nusxadan arxivlandi.
- ↑ 23,0 23,1 23,2 23,3 23,4 23,5 „Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure“. Hypertension. 42-jild, № 6. December 2003. 1206–1252-bet. doi:10.1161/01.HYP.0000107251.49515.c2. PMID 14656957.
- ↑ „Pharmacological interventions for hypertensive emergencies“. The Cochrane Database of Systematic Reviews. № 1. January 2008. CD003653-bet. doi:10.1002/14651858.CD003653.pub3. PMC 6991936. PMID 18254026.
- ↑ Harrison's principles of internal medicine., 18th, New York: McGraw-Hill, 2011 — 55–61-bet. ISBN 9780071748896.
- ↑ 26,0 26,1 „Management of hypertension in pregnant and postpartum women“. www.uptodate.com. 2016-yil 4-martda asl nusxadan arxivlangan. Qaraldi: 2015-yil 30-iyul.
- ↑ „Hypertension and Pregnancy“. eMedicine Obstetrics and Gynecology. Medscape (2009-yil 30-iyul). 2009-yil 24-iyulda asl nusxadan arxivlangan. Qaraldi: 2009-yil 16-iyun.
- ↑ 28,0 28,1 „Hypertension“. eMedicine Pediatrics: Cardiac Disease and Critical Care Medicine. Medscape (2010-yil 6-aprel). 2009-yil 15-avgustda asl nusxadan arxivlangan. Qaraldi: 2009-yil 16-iyun.
- ↑ 29,0 29,1 29,2 „Hypertension in infancy: diagnosis, management and outcome“. Pediatric Nephrology. 27-jild, № 1. January 2012. 17–32-bet. doi:10.1007/s00467-010-1755-z. PMID 21258818.
- ↑ „Genetic variants in novel pathways influence blood pressure and cardiovascular disease risk“. Nature. 478-jild, № 7367. September 2011. 103–109-bet. Bibcode:2011Natur.478..103T. doi:10.1038/nature10405. PMC 3340926. PMID 21909115.
- ↑ „Molecular mechanisms of human hypertension“. Cell. 104-jild, № 4. February 2001. 545–556-bet. doi:10.1016/S0092-8674(01)00241-0. PMID 11239411.
- ↑ 32,0 32,1 „Trans-ancestry genome-wide association study identifies 12 genetic loci influencing blood pressure and implicates a role for DNA methylation“. Nature Genetics. 47-jild, № 11. November 2015. 1282–1293-bet. doi:10.1038/ng.3405. PMC 4719169. PMID 26390057.
- ↑ „Residual lifetime risk for developing hypertension in middle-aged women and men: The Framingham Heart Study“. JAMA. 287-jild, № 8. February 2002. 1003–1010-bet. doi:10.1001/jama.287.8.1003. PMID 11866648.
- ↑ „The western diet and lifestyle and diseases of civilization“. Research Reports in Clinical Cardiology (English). 2-jild. 2011-03-09. 15–35-bet. doi:10.2147/RRCC.S16919. Qaraldi: 2021-02-09.
{{cite magazine}}: CS1 maint: unrecognized language () - ↑ „The effect of coffee on blood pressure and cardiovascular disease in hypertensive individuals: a systematic review and meta-analysis“. The American Journal of Clinical Nutrition. 94-jild, № 4. October 2011. 1113–1126-bet. doi:10.3945/ajcn.111.016667. PMID 21880846.
- ↑ „Vitamin D and hypertension: current evidence and future directions“. Hypertension. 56-jild, № 5. November 2010. 774–779-bet. doi:10.1161/HYPERTENSIONAHA.109.140160. PMID 20937970.
- ↑ „Obesity hypertension in children: a problem of epidemic proportions“. Hypertension. 40-jild, № 4. October 2002. 441–447-bet. doi:10.1161/01.HYP.0000032940.33466.12. PMID 12364344.
- ↑ „Pharmacotherapy for hyperuricaemia in hypertensive patients“. The Cochrane Database of Systematic Reviews. 2020-jild, № 9. September 2020. CD008652-bet. doi:10.1002/14651858.CD008652.pub4. PMC 8094453. PMID 32877573.
- ↑ „Winter Hypertension: Potential mechanisms“. International Journal of Health Sciences. 7-jild, № 2. June 2013. 210–219-bet. doi:10.12816/0006044. PMC 3883610. PMID 24421749.
- ↑ „Periodontitis is associated with hypertension: a systematic review and meta-analysis“. Cardiovascular Research. 116-jild, № 1. January 2020. 28–39-bet. doi:10.1093/cvr/cvz201. PMID 31549149.
{{cite magazine}}: Invalid|display-authors=6(yordam) - ↑ „Endocrine hypertension“, Williams textbook of endocrinology, 9th, Philadelphia; Montreal: W.B. Saunders, 1998 — 729–749-bet. ISBN 978-0721661520.
- ↑ „Drug-induced hypertension: an unappreciated cause of secondary hypertension“. The American Journal of Medicine. 125-jild, № 1. January 2012. 14–22-bet. doi:10.1016/j.amjmed.2011.05.024. PMID 22195528.
- ↑ „Association between Arsenic Exposure from Drinking Water and Longitudinal Change in Blood Pressure among HEALS Cohort Participants“. Environmental Health Perspectives. 123-jild, № 8. August 2015. 806–812-bet. doi:10.1289/ehp.1409004. PMC 4529016. PMID 25816368.
- ↑ „Arsenic exposure and hypertension: a systematic review“. Environmental Health Perspectives. 120-jild, № 4. April 2012. 494–500-bet. doi:10.1289/ehp.1103988. PMC 3339454. PMID 22138666.
- ↑ „Depression increases the risk of hypertension incidence: a meta-analysis of prospective cohort studies“. Journal of Hypertension. 30-jild, № 5. May 2012. 842–851-bet. doi:10.1097/hjh.0b013e32835080b7. PMID 22343537.
- ↑ „Loneliness matters: a theoretical and empirical review of consequences and mechanisms“. Annals of Behavioral Medicine. 40-jild, № 2. October 2010. 218–227-bet. doi:10.1007/s12160-010-9210-8. PMC 3874845. PMID 20652462.
- ↑ „Sex-Specific Associations Between Alcohol Consumption and Incidence of Hypertension: A Systematic Review and Meta-Analysis of Cohort Studies“. Journal of the American Heart Association. 7-jild, № 13. June 2018. e008202-bet. doi:10.1161/JAHA.117.008202. PMC 6064910. PMID 29950485.
- ↑ „Hemodynamic aspects of essential hypertension in humans“. Physiological Reviews. 64-jild, № 2. April 1984. 617–660-bet. doi:10.1152/physrev.1984.64.2.617. PMID 6369352.
- ↑ 49,0 49,1 „The role of cardiac autonomic function in hypertension and cardiovascular disease“. Current Hypertension Reports. 11-jild, № 3. June 2009. 199–205-bet. doi:10.1007/s11906-009-0035-4. PMID 19442329.
- ↑ „Physiological aspects of primary hypertension“. Physiological Reviews. 62-jild, № 2. April 1982. 347–504-bet. doi:10.1152/physrev.1982.62.2.347. PMID 6461865.
- ↑ „The microcirculation and hypertension“. Journal of Hypertension Supplement. 10-jild, № 7. December 1992. S147–156-bet. doi:10.1097/00004872-199212000-00016. PMID 1291649.
- ↑ „Arterial and venous compliance in sustained essential hypertension“. Hypertension. 10-jild, № 2. August 1987. 133–139-bet. doi:10.1161/01.HYP.10.2.133. PMID 3301662.
- ↑ Steppan, Jochen; Barodka, Viachaslau; Berkowitz, Dan E.; Nyhan, Daniel (2011-08-02). „Vascular Stiffness and Increased Pulse Pressure in the Aging Cardiovascular System“. Cardiology Research and Practice. 2011-jild. 263585-bet. doi:10.4061/2011/263585. ISSN 2090-8016. PMC 3154449. PMID 21845218.
- ↑ „Clinical practice. Isolated systolic hypertension in the elderly“. The New England Journal of Medicine. 357-jild, № 8. August 2007. 789–796-bet. doi:10.1056/NEJMcp071137. PMID 17715411.
- ↑ „Mechanisms, pathophysiology, and therapy of arterial stiffness“. Arteriosclerosis, Thrombosis, and Vascular Biology. 25-jild, № 5. May 2005. 932–943-bet. doi:10.1161/01.ATV.0000160548.78317.29. PMID 15731494.
- ↑ „Counterpoint: Activation of the intrarenal renin-angiotensin system is the dominant contributor to systemic hypertension“. Journal of Applied Physiology. 109-jild, № 6. December 2010. 1998–2000, discussion 2015-bet. doi:10.1152/japplphysiol.00182.2010a. PMC 3006411. PMID 21148349.
- ↑ „Point: Chronic activation of the sympathetic nervous system is the dominant contributor to systemic hypertension“. Journal of Applied Physiology. 109-jild, № 6. December 2010. 1996–1998, discussion 2016-bet. doi:10.1152/japplphysiol.00182.2010. PMID 20185633.
- ↑ „Endothelium-dependent contractions and endothelial dysfunction in human hypertension“. British Journal of Pharmacology. 157-jild, № 4. June 2009. 527–536-bet. doi:10.1111/j.1476-5381.2009.00240.x. PMC 2707964. PMID 19630832.
- ↑ „Role of the renin-angiotensin system in vascular inflammation“. Trends in Pharmacological Sciences. 29-jild, № 7. July 2008. 367–374-bet. doi:10.1016/j.tips.2008.05.003. PMID 18579222.
- ↑ „Targeting the immune system to treat hypertension: where are we?“. Current Opinion in Nephrology and Hypertension. 23-jild, № 5. September 2014. 473–479-bet. doi:10.1097/MNH.0000000000000052. PMID 25036747.
- ↑ „Sodium and potassium in the pathogenesis of hypertension“. The New England Journal of Medicine. 356-jild, № 19. May 2007. 1966–1978-bet. doi:10.1056/NEJMra064486. PMID 17494929.
- ↑ „Sodium-to-potassium ratio and blood pressure, hypertension, and related factors“. Advances in Nutrition. 5-jild, № 6. November 2014. 712–741-bet. doi:10.3945/an.114.006783. PMC 4224208. PMID 25398734.
- ↑ „ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents developed in collaboration with the American Academy of Neurology, American Geriatrics Society, American Society for Preventive Cardiology, American Society of Hypertension, American Society of Nephrology, Association of Black Cardiologists, and European Society of Hypertension“. Journal of the American Society of Hypertension. 5-jild, № 4. 2011. 259–352-bet. doi:10.1016/j.jash.2011.06.001. PMID 21771565.
- ↑ „Hypertension in adults: diagnosis and management | Guidance and guidelines | NICE“. www.nice.org.uk. 2017-yil 9-aprelda asl nusxadan arxivlangan. Qaraldi: 2018-yil 11-noyabr.
- ↑ 65,0 65,1 65,2 65,3 65,4 65,5 65,6 „Screening for Hypertension and Lowering Blood Pressure for Prevention of Cardiovascular Disease Events“. The Medical Clinics of North America. 101-jild, № 4. July 2017. 701–712-bet. doi:10.1016/j.mcna.2017.03.003. PMID 28577621.
- ↑ 66,0 66,1 66,2 Principles of Blood Pressure Measurement – Current Techniques, Office vs Ambulatory Blood Pressure Measurement, 2017 — 85–96-bet. DOI:10.1007/5584_2016_49. ISBN 978-3-319-44250-1.
- ↑ 67,0 67,1 „Screening for high blood pressure in adults: U.S. Preventive Services Task Force recommendation statement“. Annals of Internal Medicine. 163-jild, № 10. November 2015. 778–786-bet. doi:10.7326/m15-2223. PMID 26458123.
- ↑ National Clinical Guidance Centre „7 Diagnosis of Hypertension, 7.5 Link from evidence to recommendations“, . Hypertension (NICE CG 127). National Institute for Health and Clinical Excellence, August 2011 — 102-bet. (Wayback Machine saytida 2013-07-23 sanasida arxivlangan)
- ↑ „Unusual hypertensive phenotypes: what is their significance?“. Hypertension. 59-jild, № 2. February 2012. 173–178-bet. doi:10.1161/HYPERTENSIONAHA.111.182956. PMID 22184330.
- ↑ „Orthostatic hypertension: a measure of blood pressure variation for predicting cardiovascular risk“. Circulation Journal. 73-jild, № 6. June 2009. 1002–1007-bet. doi:10.1253/circj.cj-09-0286. PMID 19430163.
- ↑ Harrison's principles of internal medicine. McGraw-Hill Medical, 2008. ISBN 978-0-07-147691-1.
- ↑ „The 2009 Canadian Hypertension Education Program recommendations for the management of hypertension: Part 1 – blood pressure measurement, diagnosis and assessment of risk“. The Canadian Journal of Cardiology. 25-jild, № 5. May 2009. 279–286-bet. doi:10.1016/S0828-282X(09)70491-X. PMC 2707176. PMID 19417858.
- ↑ „The 2008 Canadian Hypertension Education Program recommendations for the management of hypertension: Part 1 – blood pressure measurement, diagnosis and assessment of risk“. The Canadian Journal of Cardiology. 24-jild, № 6. June 2008. 455–463-bet. doi:10.1016/S0828-282X(08)70619-6. PMC 2643189. PMID 18548142.
- ↑ „The 2007 Canadian Hypertension Education Program recommendations for the management of hypertension: part 1 – blood pressure measurement, diagnosis and assessment of risk“. The Canadian Journal of Cardiology. 23-jild, № 7. May 2007. 529–538-bet. doi:10.1016/S0828-282X(07)70797-3. PMC 2650756. PMID 17534459.
- ↑ „The 2006 Canadian Hypertension Education Program recommendations for the management of hypertension: Part I – Blood pressure measurement, diagnosis and assessment of risk“. The Canadian Journal of Cardiology. 22-jild, № 7. May 2006. 573–581-bet. doi:10.1016/S0828-282X(06)70279-3. PMC 2560864. PMID 16755312.
- ↑ „The 2005 Canadian Hypertension Education Program recommendations for the management of hypertension: part 1 – blood pressure measurement, diagnosis and assessment of risk“. The Canadian Journal of Cardiology. 21-jild, № 8. June 2005. 645–656-bet. PMID 16003448.
- ↑ „Hypertension in children and adolescents“. American Family Physician. 73-jild, № 9. May 2006. 1558–1568-bet. PMID 16719248.
- ↑ 78,0 78,1 78,2 78,3 78,4 78,5 78,6 78,7 „Guideline for the diagnosis and management of hypertension in adults“ 12. Heart Foundation (2016). 2017-yil 14-yanvarda asl nusxadan arxivlangan. Qaraldi: 2017-yil 12-yanvar.
- ↑ 79,0 79,1 „AAFP Decides to Not Endorse AHA/ACC Hypertension Guideline“. AAFP (2017-yil 12-dekabr). 2018-yil 7-yanvarda asl nusxadan arxivlangan. Qaraldi: 2017-yil 15-dekabr.
- ↑ „[Isolated diastolic hypertension : do we still have to care about it ?]“. Revue Médicale Suisse. 14-jild, № 618. September 2018. 1607–1610-bet. doi:10.53738/REVMED.2018.14.618.1607. PMID 30226658. 22 May 2020da asl nusxadan arxivlandi.
{{cite magazine}}: Unknown parameter|trans_title=ignored (|trans-title=suggested) (yordam) - ↑ „Isolated diastolic hypertension“. Journal of Clinical Hypertension. 5-jild, № 6. Wiley. 2003. 411–413-bet. doi:10.1111/j.1524-6175.2003.02840.x. PMC 8099308. PMID 14688497.
- ↑ „2007 ESH-ESC Practice Guidelines for the Management of Arterial Hypertension: ESH-ESC Task Force on the Management of Arterial Hypertension“. Journal of Hypertension. 25-jild, № 9. September 2007. 1751–1762-bet. doi:10.1097/HJH.0b013e3282f0580f. PMID 17762635.
- ↑ 83,0 83,1 „Guidelines for management of hypertension: report of the fourth working party of the British Hypertension Society, 2004-BHS IV“. Journal of Human Hypertension. 18-jild, № 3. March 2004. 139–185-bet. doi:10.1038/sj.jhh.1001683. PMID 14973512.
- ↑ „2017 Guideline for High Blood Pressure in Adults“. American College of Cardiology. 19 November 2017da asl nusxadan arxivlandi. Qaraldi: 21 November 2017.
- ↑ „2020 International Society of Hypertension Global Hypertension Practice Guidelines“. Hypertension. 75-jild, № 6. June 2020. 1334–1357-bet. doi:10.1161/HYPERTENSIONAHA.120.15026. PMID 32370572.
{{cite magazine}}: Invalid|display-authors=6(yordam) - ↑ 86,0 86,1 86,2 86,3 National High Blood Pressure Education Program Working Group on High Blood Pressure in Children Adolescents (August 2004). „The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents“. Pediatrics. 114-jild, № 2 Suppl 4th Report. 555–576-bet. doi:10.1542/peds.114.2.S2.555. PMID 15286277.
- ↑ Expert Panel on Integrated Guidelines for Cardiovascular Health Risk Reduction in Children Adolescents; National Heart, Lung, and Blood Institute (December 2011). „Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report“. Pediatrics. 128-jild, № Suppl 5. S213–256-bet. doi:10.1542/peds.2009-2107C. PMC 4536582. PMID 22084329.
{{cite magazine}}: CS1 maint: multiple names: authors list () - ↑ „Hypertension - Clinical Preventive Service Recommendation“. 2014-yil 1-noyabrda asl nusxadan arxivlangan. Qaraldi: 2013-yil 13-oktyabr.
- ↑ „Screening for primary hypertension in children and adolescents: U.S. Preventive Services Task Force recommendation statement“. Annals of Internal Medicine. 159-jild, № 9. November 2013. 613–619-bet. doi:10.7326/0003-4819-159-9-201311050-00725. PMID 24097285.
- ↑ „Document | United States Preventive Services Taskforce“. www.uspreventiveservicestaskforce.org. 2020-yil 22-mayda asl nusxadan arxivlangan. Qaraldi: 2020-yil 22-aprel.
- ↑ „Primary prevention of hypertension: clinical and public health advisory from The National High Blood Pressure Education Program“. JAMA. 288-jild, № 15. October 2002. 1882–1888-bet. doi:10.1001/jama.288.15.1882. PMID 12377087.
- ↑ 92,0 92,1 „Hypertension: Causes, symptoms, and treatments“ (en). www.medicalnewstoday.com (2021-yil 10-noyabr). Qaraldi: 2022-yil 27-aprel.
- ↑ 93,0 93,1 „Evidence-based policy for salt reduction is needed“. Lancet. 388-jild, № 10043. July 2016. 438-bet. doi:10.1016/S0140-6736(16)31205-3. PMID 27507743.
- ↑ „Associations of urinary sodium excretion with cardiovascular events in individuals with and without hypertension: a pooled analysis of data from four studies“. Lancet. 388-jild, № 10043. July 2016. 464–475-bet. doi:10.1016/S0140-6736(16)30467-6. PMID 27216139. „The results showed that cardiovascular disease and death are increased with low sodium intake (compared with moderate intake) irrespective of hypertension status, whereas there is a higher risk of cardiovascular disease and death only in individuals with hypertension consuming more than 6 g of sodium per day (representing only 10% of the population studied)“
- ↑ „European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts)“. European Heart Journal. 33-jild, № 13. July 2012. 1635–1701-bet. doi:10.1093/eurheartj/ehs092. PMID 22555213.
- ↑ „Lowering blood pressure to prevent myocardial infarction and stroke: a new preventive strategy“. Health Technology Assessment. 7-jild, № 31. 2003. 1–94-bet. doi:10.3310/hta7310. PMID 14604498.
- ↑ 97,0 97,1 „The 2015 Canadian Hypertension Education Program recommendations for blood pressure measurement, diagnosis, assessment of risk, prevention, and treatment of hypertension“. The Canadian Journal of Cardiology. 31-jild, № 5. May 2015. 549–568-bet. doi:10.1016/j.cjca.2015.02.016. PMID 25936483.
- ↑ 98,0 98,1 „Hypertension: Recommendations, Guidance and guidelines“. NICE. 2006-yil 3-oktyabrda asl nusxadan arxivlangan. Qaraldi: 2015-yil 4-avgust.
- ↑ 99,0 99,1 „Blood pressure targets for hypertension in people with diabetes mellitus“. The Cochrane Database of Systematic Reviews. № 10. October 2013. CD008277-bet. doi:10.1002/14651858.cd008277.pub2. PMID 24170669.
- ↑ „Blood pressure targets for the treatment of people with hypertension and cardiovascular disease“. The Cochrane Database of Systematic Reviews. 2020-jild, № 9. September 2020. CD010315-bet. doi:10.1002/14651858.CD010315.pub4. PMC 8094921. PMID 32905623.
- ↑ 101,0 101,1 „Blood pressure targets in adults with hypertension“. The Cochrane Database of Systematic Reviews. 2020-jild, № 12. December 2020. CD004349-bet. doi:10.1002/14651858.CD004349.pub3. PMC 8094587. PMID 33332584.
- ↑ „Pharmacologic Treatment of Hypertension in Adults Aged 60 Years or Older to Higher Versus Lower Blood Pressure Targets: A Clinical Practice Guideline From the American College of Physicians and the American Academy of Family Physicians“. Annals of Internal Medicine. 166-jild, № 6. March 2017. 430–437-bet. doi:10.7326/M16-1785. PMID 28135725.
- ↑ „Pharmacologic Treatment of Hypertension in Adults Aged 60 Years or Older to Higher Versus Lower Blood Pressure Targets: A Clinical Practice Guideline From the American College of Physicians and the American Academy of Family Physicians“. Annals of Internal Medicine. 166-jild, № 6. March 2017. 430–437-bet. doi:10.7326/m16-1785. PMID 28135725.
- ↑ „Evidence supporting a systolic blood pressure goal of less than 150 mm Hg in patients aged 60 years or older: the minority view“. Annals of Internal Medicine. 160-jild, № 7. April 2014. 499–503-bet. doi:10.7326/m13-2981. PMID 24424788.
- ↑ „KDIGO Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease“ (PDF). Kidney International Supplements. December 2012. 16 June 2015da asl nusxadan (PDF) arxivlandi.
- ↑ „Lower blood pressure targets: to whom do they apply?“. Lancet. 387-jild, № 10017. January 2016. 405–406-bet. doi:10.1016/S0140-6736(15)00816-8. PMID 26559745.
- ↑ „Long-term effects of weight-reducing diets in people with hypertension“. The Cochrane Database of Systematic Reviews. 2021-jild, № 2. February 2021. CD008274-bet. doi:10.1002/14651858.CD008274.pub4. PMC 8093137. PMID 33555049.
- ↑ „Effect of longer-term modest salt reduction on blood pressure“. The Cochrane Database of Systematic Reviews. 30-jild, № 4. April 2013. CD004937-bet. doi:10.1002/14651858.CD004937.pub2. PMID 23633321.
- ↑ „Effect of dose and duration of reduction in dietary sodium on blood pressure levels: systematic review and meta-analysis of randomised trials“. BMJ. 368-jild. February 2020. m315-bet. doi:10.1136/bmj.m315. PMC 7190039. PMID 32094151.
{{cite magazine}}: Invalid|display-authors=6(yordam) - ↑ „Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group“. The New England Journal of Medicine. 344-jild, № 1. January 2001. 3–10-bet. doi:10.1056/NEJM200101043440101. PMID 11136953.
{{cite magazine}}: Invalid|display-authors=6(yordam) - ↑ „Plant-Based Diets and Hypertension“. American Journal of Lifestyle Medicine. 14-jild, № 4. 2020. 397–405-bet. doi:10.1177/1559827619875411. PMC 7692016. PMID 33281520.
- ↑ „Effect of green tea supplementation on blood pressure: A systematic review and meta-analysis of randomized controlled trials“. Medicine. 99-jild, № 6. February 2020. e19047-bet. doi:10.1097/MD.0000000000019047. PMC 7015560. PMID 32028419.
- ↑ „The efficacy of sour tea (Hibiscus sabdariffa L.) on selected cardiovascular disease risk factors: A systematic review and meta-analysis of randomized clinical trials“. Phytotherapy Research. 34-jild, № 2. February 2020. 329–339-bet. doi:10.1002/ptr.6541. PMID 31943427.
{{cite magazine}}: Invalid|display-authors=6(yordam) - ↑ „Hibiscus sabdariffa L. tea (tisane) lowers blood pressure in prehypertensive and mildly hypertensive adults“. The Journal of Nutrition. 140-jild, № 2. February 2010. 298–303-bet. doi:10.3945/jn.109.115097. PMID 20018807.
- ↑ „Beetroot juice lowers high blood pressure, suggests research“. British Heart Foundation.
- ↑ „Inorganic nitrate and beetroot juice supplementation reduces blood pressure in adults: a systematic review and meta-analysis“. The Journal of Nutrition. 143-jild, № 6. June 2013. 818–826-bet. doi:10.3945/jn.112.170233. PMID 23596162.
- ↑ „The Nitrate-Independent Blood Pressure-Lowering Effect of Beetroot Juice: A Systematic Review and Meta-Analysis“. Advances in Nutrition. 8-jild, № 6. November 2017. 830–838-bet. doi:10.3945/an.117.016717. PMC 5683004. PMID 29141968.
- ↑ „Effect of increased potassium intake on cardiovascular risk factors and disease: systematic review and meta-analyses“. BMJ. 346-jild. April 2013. f1378-bet. doi:10.1136/bmj.f1378. PMC 4816263. PMID 23558164.
- ↑ „Potassium Intake, Bioavailability, Hypertension, and Glucose Control“. Nutrients. 8-jild, № 7. July 2016. 444-bet. doi:10.3390/nu8070444. PMC 4963920. PMID 27455317.
- ↑ „Hyperkalemia associated with use of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers“. Cardiovascular Therapeutics. 30-jild, № 3. June 2012. e156–166-bet. doi:10.1111/j.1755-5922.2010.00258.x. PMID 21883995.
- ↑ „Beyond medications and diet: alternative approaches to lowering blood pressure: a scientific statement from the american heart association“. Hypertension. 61-jild, № 6. June 2013. 1360–1383-bet. doi:10.1161/HYP.0b013e318293645f. PMID 23608661.
- ↑ „First-line drugs for hypertension“. The Cochrane Database of Systematic Reviews. 2018-jild, № 4. April 2018. CD001841-bet. doi:10.1002/14651858.CD001841.pub3. PMC 6513559. PMID 29667175.
- ↑ „Blood pressure lowering efficacy of diuretics as second-line therapy for primary hypertension“. The Cochrane Database of Systematic Reviews. № 4. October 2009. CD007187-bet. doi:10.1002/14651858.CD007187.pub2. PMID 19821398.
- ↑ „Interventions used to improve control of blood pressure in patients with hypertension“ (PDF). The Cochrane Database of Systematic Reviews. № 3. March 2010. CD005182-bet. doi:10.1002/14651858.cd005182.pub4. PMID 20238338. 12 April 2019da asl nusxadan (PDF) arxivlandi. Qaraldi: 11 February 2019.
- ↑ „Beta-blockers for hypertension“. The Cochrane Database of Systematic Reviews. 1-jild. January 2017. CD002003-bet. doi:10.1002/14651858.CD002003.pub5. PMC 5369873. PMID 28107561.
- ↑ „Resistant hypertension: a review of diagnosis and management“ (PDF). JAMA. 311-jild, № 21. June 2014. 2216–2224-bet. doi:10.1001/jama.2014.5180. PMID 24893089. 20 April 2018da asl nusxadan (PDF) arxivlandi. Qaraldi: 19 April 2018.
- ↑ „Electronic monitors of drug adherence: tools to make rational therapeutic decisions“. Journal of Hypertension. 27-jild, № 11. November 2009. 2294–2295, author reply 2295-bet. doi:10.1097/hjh.0b013e328332a501. PMID 20724871.
- ↑ „Autonomic-immune-vascular interaction: an emerging concept for neurogenic hypertension“. Hypertension. 57-jild, № 6. June 2011. 1026–1033-bet. doi:10.1161/HYPERTENSIONAHA.111.169748. PMC 3105900. PMID 21536990.
- ↑ Sarwar, M.; Islam, M.; Al Baker, S.M.; Hasnat, A. (22 March 2013). „Resistant Hypertension: Underlying Causes and Treatment“. Drug Research. 63-jild, № 5. 217–223-bet. doi:10.1055/s-0033-1337930. PMID 23526242.
- ↑ Young, W. F. (February 2019). „Diagnosis and treatment of primary aldosteronism: practical clinical perspectives“. Journal of Internal Medicine (inglizcha). 285-jild, № 2. 126–148-bet. doi:10.1111/joim.12831. PMID 30255616.
- ↑ 131,0 131,1 „Treatment of resistant and refractory hypertension“. Circulation Research. 124-jild, № 7. March 2019. 1061–1070-bet. doi:10.1161/CIRCRESAHA.118.312156. PMC 6469348. PMID 30920924.
- ↑ „Refractory hypertension: A novel phenotype of antihypertensive treatment failure“. Hypertension. 67-jild, № 6. June 2016. 1085–1092-bet. doi:10.1161/HYPERTENSIONAHA.116.06587. PMC 5425297. PMID 27091893.
- ↑ „Blood Pressure“. World Health Organization. 2017-yil 18-aprelda asl nusxadan arxivlangan. Qaraldi: 2017-yil 22-aprel.
- ↑ „WHO Disease and injury country estimates“. World Health Organization (2009). 2009-yil 11-noyabrda asl nusxadan arxivlangan. Qaraldi: 2009-yil 11-noyabr.
- ↑ „Prevalence of hypertension in the US adult population. Results from the Third National Health and Nutrition Examination Survey, 1988–1991“. Hypertension. 25-jild, № 3. March 1995. 305–313-bet. doi:10.1161/01.HYP.25.3.305. PMID 7875754.
- ↑ 136,0 136,1 „Trends in the prevalence, awareness, treatment, and control of hypertension in the adult US population. Data from the health examination surveys, 1960 to 1991“. Hypertension. 26-jild, № 1. July 1995. 60–69-bet. doi:10.1161/01.HYP.26.1.60. PMID 7607734. 2012-12-20da asl nusxadan arxivlandi.
- ↑ „Trends in hypertension prevalence, awareness, treatment, and control in older U.S. adults: data from the National Health and Nutrition Examination Survey 1988 to 2004“. Journal of the American Geriatrics Society. 55-jild, № 7. July 2007. 1056–1065-bet. doi:10.1111/j.1532-5415.2007.01215.x. PMID 17608879.
- ↑ 138,0 138,1 138,2 „Heart disease and stroke statistics – 2010 update: a report from the American Heart Association“. Circulation. 121-jild, № 7. February 2010. e46–e215-bet. doi:10.1161/CIRCULATIONAHA.109.192667. PMID 20019324.
- ↑ „Culture-Specific of Health Risk Health Status: Morbidity and Mortality“. Stanford (2014-yil 16-mart). 2016-yil 15-fevralda asl nusxadan arxivlangan. Qaraldi: 2016-yil 12-aprel.
- ↑ „Epidemiological issues are not simply black and white“. Hypertension. 58-jild, № 4. October 2011. 546–547-bet. doi:10.1161/HYPERTENSIONAHA.111.178541. PMID 21911712.
- ↑ „Hypertension in children and adolescents: epidemiology and natural history“. Pediatric Nephrology. 25-jild, № 7. July 2010. 1219–1224-bet. doi:10.1007/s00467-009-1200-3. PMC 2874036. PMID 19421783.
- ↑ „Hypertension in children and adolescents“. American Family Physician. 73-jild, № 9. May 2006. 1558–1568-bet. PMID 16719248. 26 September 2007da asl nusxadan arxivlandi.
- ↑ „Global health risks: mortality and burden of disease attributable to selected major risks“. World Health Organization (2009). 2012-yil 14-fevralda asl nusxadan arxivlangan. Qaraldi: 2012-yil 10-fevral.
- ↑ „Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies“. Lancet. 360-jild, № 9349. December 2002. 1903–1913-bet. doi:10.1016/S0140-6736(02)11911-8. PMID 12493255.
- ↑ „Management of hypertension in peripheral arterial disease: does the choice of drugs matter?“. European Journal of Vascular and Endovascular Surgery. 35-jild, № 6. June 2008. 701–708-bet. doi:10.1016/j.ejvs.2008.01.007. PMID 18375152.
- ↑ 146,0 146,1 146,2 146,3 146,4 146,5 146,6 146,7 „From blood pressure to hypertension: the history of research“. Journal of the Royal Society of Medicine. 84-jild, № 10. October 1991. 621-bet. doi:10.1177/014107689108401019. PMC 1295564. PMID 1744849.
- ↑ 147,0 147,1 „Historical trends and milestones in hypertension research: a model of the process of translational research“. Hypertension. 58-jild, № 4. October 2011. 522–38-bet. doi:10.1161/HYPERTENSIONAHA.111.177766. PMID 21859967.
- ↑ A century of arterial hypertension 1896–1996 Postel-Vinay N: . Chichester: Wiley, 1996 — 213-bet. ISBN 978-0-471-96788-0.
- ↑ „The medieval origins of the concept of hypertension“. Heart Views. 15-jild, № 3. July 2014. 96–98-bet. doi:10.4103/1995-705X.144807. PMC 4268622. PMID 25538828.
- ↑ „Avicenna's doctrine about arterial hypertension“. Acta Medico-Historica Adriatica. 12-jild, № 1. 2014. 157–162-bet. PMID 25310615.
- ↑ Manual of hypertension Swales JD: . Oxford: Blackwell Science, 1995 — xiii-bet. ISBN 978-0-86542-861-4.
- ↑ 152,0 152,1 „Controlling hypertension. A research success story“. Archives of Internal Medicine. 156-jild, № 17. September 1996. 1926–1935-bet. doi:10.1001/archinte.156.17.1926. PMID 8823146.
- ↑ „Experiences with tetraethylammonium chloride in hypertension“. Journal of the American Medical Association. 136-jild, № 9. February 1948. 608–613-bet. doi:10.1001/jama.1948.02890260016005. PMID 18899127.
- ↑ „The evolution of antihypertensive therapy: an overview of four decades of experience“. Journal of the American College of Cardiology. 14-jild, № 7. December 1989. 1595–1608-bet. doi:10.1016/0735-1097(89)90002-8. PMID 2685075.
- ↑ „Benzothiadiazine dioxides as novel diuretics“. J. Am. Chem. Soc. 79-jild, № 8. 1957. 2028–2029-bet. doi:10.1021/ja01565a079.
- ↑ 156,0 156,1 „Impact of World Hypertension Day“. The Canadian Journal of Cardiology. 23-jild, № 7. May 2007. 517–519-bet. doi:10.1016/S0828-282X(07)70795-X. PMC 2650754. PMID 17534457.
- ↑ „Hypertension, a health economics perspective“. Therapeutic Advances in Cardiovascular Disease. 2-jild, № 3. June 2008. 147–155-bet. doi:10.1177/1753944708090572. PMID 19124418.
- ↑ „The economic impact of hypertension“. Journal of Clinical Hypertension. 5-jild, № 3 Suppl 2. October 2003. 3–13-bet. doi:10.1111/j.1524-6175.2003.02463.x. PMC 8099256. PMID 12826765.
- ↑ „Economic benefits of treating high-risk hypertension with angiotensin II receptor antagonists (blockers)“. Clinical Drug Investigation. 28-jild, № 4. 2008. 211–220-bet. doi:10.2165/00044011-200828040-00002. PMID 18345711.
- ↑ „ISFM Consensus Guidelines on the Diagnosis and Management of Hypertension in Cats“. Journal of Feline Medicine and Surgery. 19-jild, № 3. March 2017. 288–303-bet. doi:10.1177/1098612X17693500. PMID 28245741.
- ↑ „ACVIM consensus statement: Guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats“. Journal of Veterinary Internal Medicine. 32-jild, № 6. November 2018. 1803–1822-bet. doi:10.1111/jvim.15331. PMC 6271319. PMID 30353952.